The 47% Who Never Get the Injection Have Always Been the Real Problem
LAI-PrEP is >96% effective. Nearly half of prescribed patients never receive it. This project redefines where the PrEP cascade fails — and what to do about it.
Long-acting injectable cabotegravir (LAI-CAB) demonstrated 66–89% superior efficacy over daily oral TDF/FTC in landmark trials (HPTN 083, HPTN 084, PURPOSE-1, PURPOSE-2) across more than 15,000 participants. It eliminates the daily adherence burden that drives oral PrEP failure.
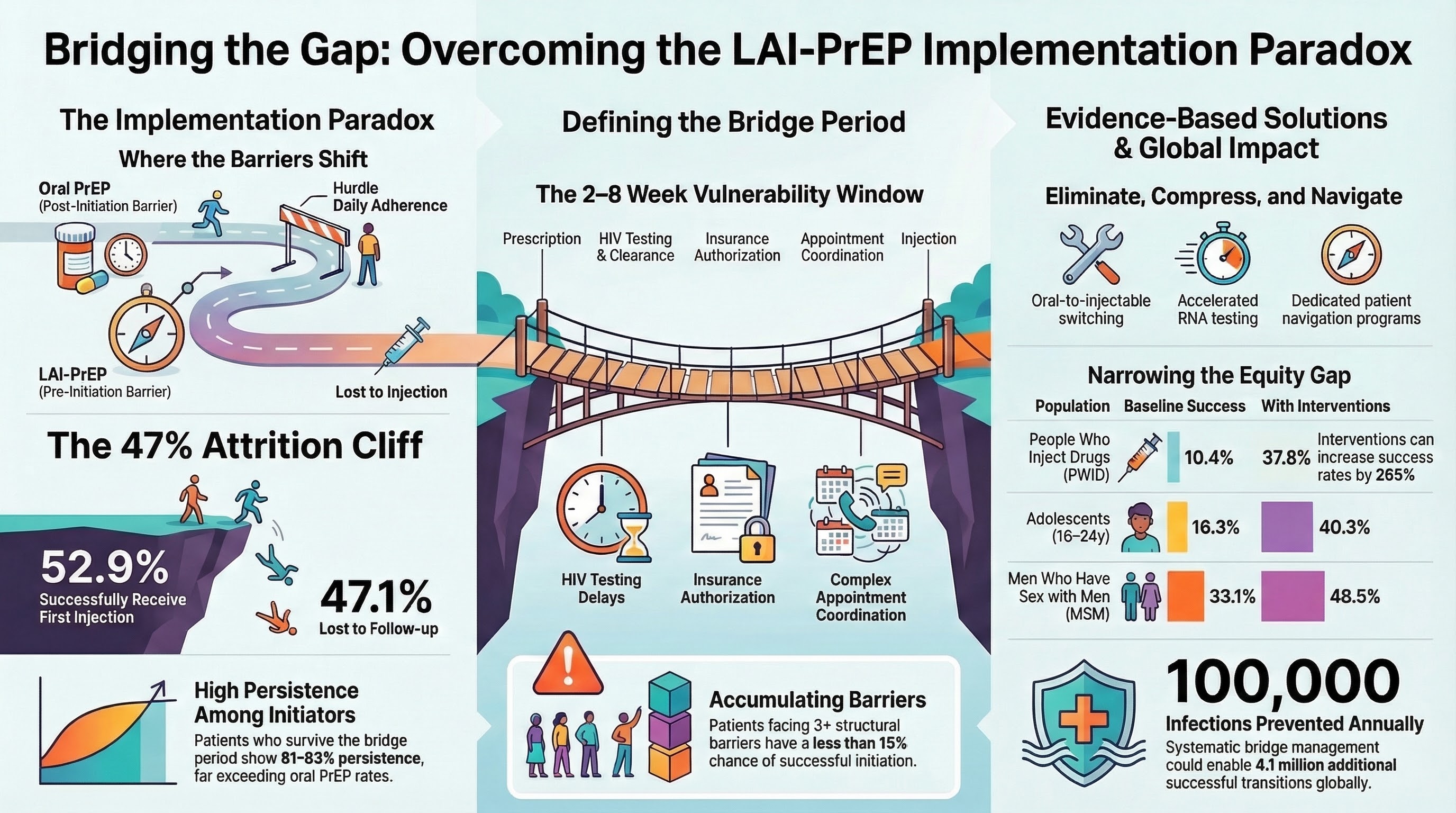
But unlike oral PrEP — which can be started the same day after a negative HIV test — LAI-PrEP cannot. Guidelines require confirmed HIV-negative status within 7 days before each injection. This creates a mandatory 2–8 week gap between prescription and first injection: the bridge period. And nearly half of patients fall into it.
>96%
HIV prevention efficacy in clinical trials
47.1%
Patients prescribed LAI-PrEP who never receive first injection
2–8 wk
Bridge period vulnerability window
81–85%
12-month persistence among those who initiate
This is the cascade paradox: LAI-PrEP solves the post-initiation adherence problem that kills oral PrEP, but introduces a new pre-initiation attrition cliff that is 2.4× higher than oral PrEP early discontinuation. The failure point has moved — and the clinical infrastructure hasn't caught up.
02 — Reconceptualized Cascade
Where LAI-PrEP Actually Fails
Traditional PrEP cascade models measure failure at adherence. For LAI-PrEP, the primary bottleneck is pre-initiation. The bridge period compresses multiple structural barriers into a single high-risk window.
Step 1
Prescription
Provider prescribes LAI-PrEP. Clock starts. Patient has 2–8 weeks to navigate everything below.
Step 2
HIV Testing & Clearance
Must confirm HIV-negative within 7 days before injection. Standard rapid tests can miss acute infection — RNA testing required in high-risk scenarios, adding 24–48 hours minimum.
Step 3
Insurance Authorization
Prior authorization requirements vary by payer and state. Delays of days to weeks are common. Uninsured patients face full out-of-pocket costs without navigation support.
Step 4
Appointment Coordination
Injection must be administered by a provider — unlike oral PrEP, which can be dispensed at a pharmacy. Scheduling, transportation, and clinic capacity all create friction.
Cliff
Lost to Injection (47.1%)
Patients facing 3+ structural barriers have <15% chance of successful initiation. Each additional barrier compounds the attrition multiplicatively.
Patients who clear this gauntlet show persistence rates (81–85% at 12 months) far exceeding oral PrEP (~50%). The drug isn't the problem. The system between prescription and injection is.
03 — Population-Specific Barriers
Structural Barriers Drive a Profound Equity Crisis
Bridge period attrition falls hardest on populations already underserved by the oral PrEP cascade. Baseline success rates reflect structural disadvantage — not individual behavior.
People Who Inject Drugs (PWID)
Baseline10.4%
With interventions37.8%
+265% relative improvement. Criminalization, housing instability, and stigma compound. SSP integration is primary pathway.
Highest baseline. Stigma and appointment coordination remain key barriers even in well-resourced settings.
Sub-Saharan Africa
Regional baseline21.7%
Europe / Central Asia29.3%
Serves 62% of global PrEP patients. 7.6 pp regional disparity despite serving the highest-burden populations.
Evidence-based interventions disproportionately benefit vulnerable populations — they narrow, not widen, health equity gaps at scale. Systematic support narrows rather than widens equity gaps.
04 — The Clinical Decision Support Tool
An Engine of 21 Evidence-Based Interventions
The tool operates across three complementary mechanisms synthesized from major LAI-PrEP trials and real-world implementation data. It functions as a clinician-guided support system — not an autonomous decision engine.
At UNAIDS 21.2 million PrEP target scale · ±0.018 pp precision
05 — Computational Validation
Policy-Grade Precision at UNAIDS Scale
Progressive validation across four scales demonstrates convergence and increasing precision — exactly the pattern expected from a well-specified model. The final validation at 21.2 million patients matches the exact UNAIDS 2025 PrEP target, making predictions directly policy-relevant.
1K
Functional validation · ±2.6 pp
1M
Large-scale · ±0.09 pp
10M
Ultra-large-scale · ±0.028 pp
21.2M
UNAIDS target scale · ±0.018 pp
The ±0.018 pp margin at 21.2M scale is not a clinical estimate — it is policy-grade statistical precision, suitable for informing WHO and UNAIDS resource allocation decisions. Unit testing achieved 100% pass rate (18/18 edge cases) including maximum barriers, extremes of age, and resource-limited settings.
4.1 million additional successful transitions at UNAIDS scale23.4% of gap closed
~100,000 HIV infections prevented annually (midpoint)5-year projection
USD $40 billion in averted lifetime treatment costs11:1 ROI
7 populations · 5 regions · 8 healthcare settings · 18/18 edge case pass rate · External validation against published real-world implementation cohorts · Largest computational validation of any HIV prevention tool to date (to our knowledge)
Demidont AC. Computational Validation of a Clinical Decision Support Algorithm for LAI-PrEP Bridge Period Navigation at UNAIDS PrEP Target Scale (21.2 Million Individuals). Viruses 2026, 18, 237. doi: 10.3390/v18020237
BibTeX
@article{Demidont2026laip, author = {Demidont, A.C.}, title = {Computational Validation of a Clinical Decision Support Algorithm for LAI-PrEP Bridge Period Navigation at UNAIDS PrEP Target Scale (21.2 Million Individuals)}, journal = {Viruses}, year = {2026}, volume = {18}, number = {2}, pages = {237}, doi = {10.3390/v18020237} }
Companion Preprint
Demidont AC. LAI-PrEP Bridge Period Navigation: Reconceptualized Cascade and Implementation Framework. Preprints.org 2025. doi: 10.20944/preprints202512.2354.v1