Slide 01 — The Central Claim
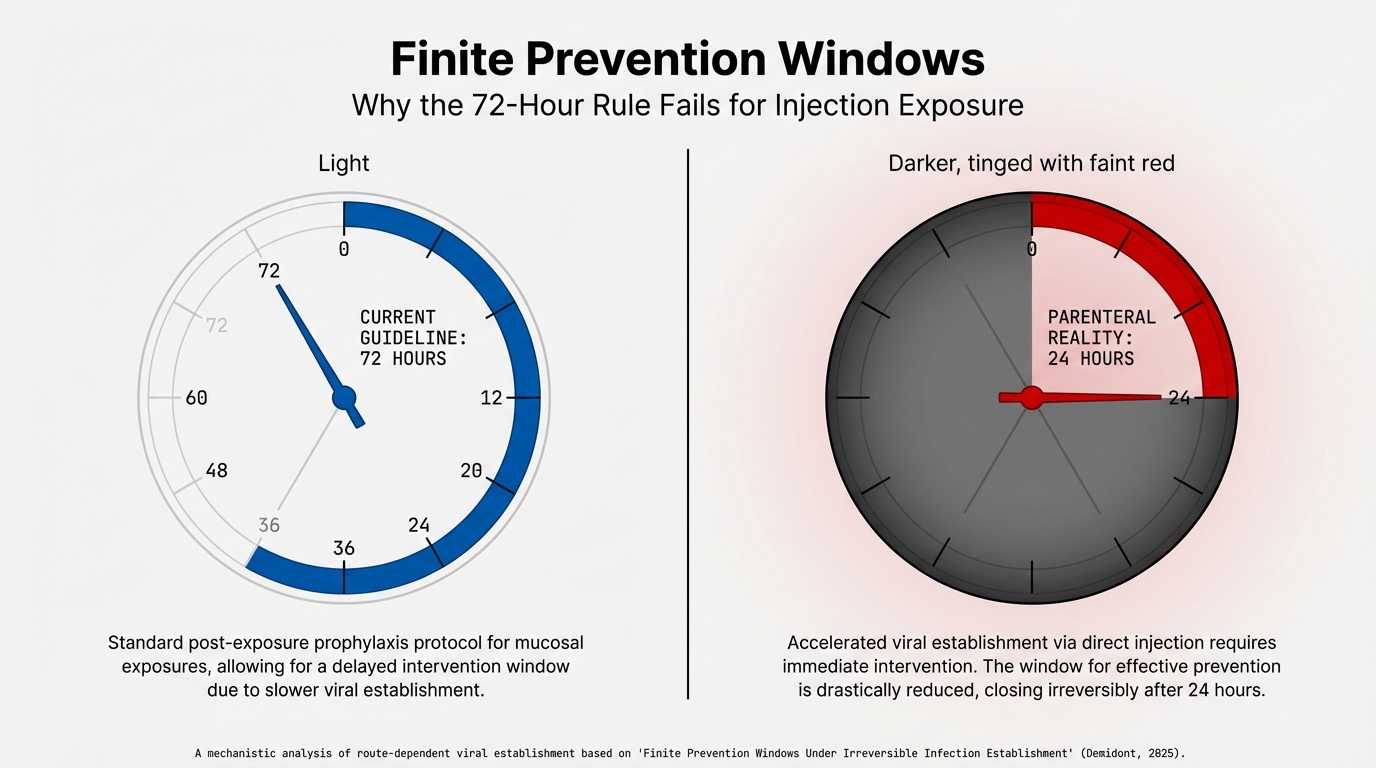
The 72-hour PEP window is an artifact of mucosal transmission. For parenteral (injection) exposure, accelerated viral establishment compresses the effective window to ~16–28 hours. The standard guideline does not apply.
Slide 02 — The Current Paradigm
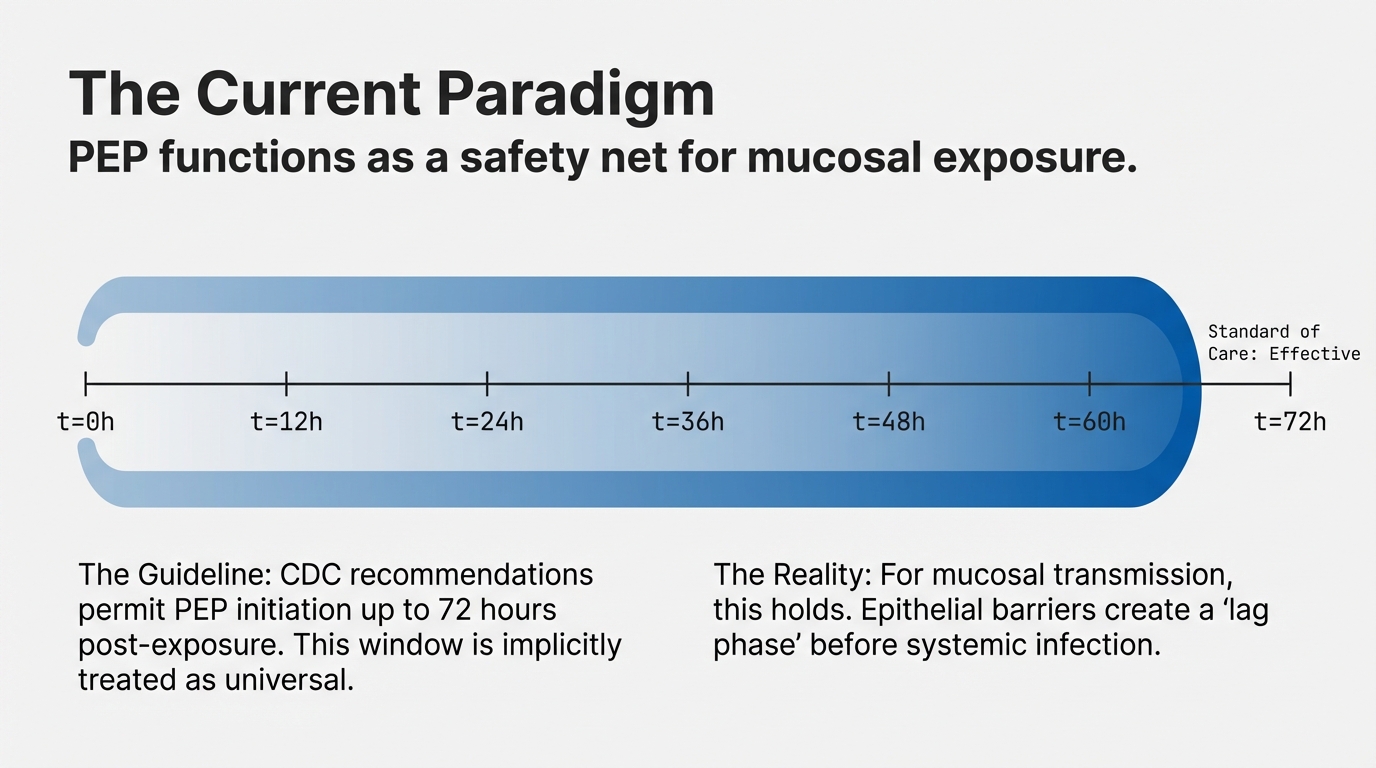
CDC guidelines permit PEP initiation up to 72 hours post-exposure. This window is implicitly treated as universal, but it was derived from mucosal transmission dynamics where epithelial barriers create a “lag phase” before systemic infection.
Slide 03 — The Absorbing State
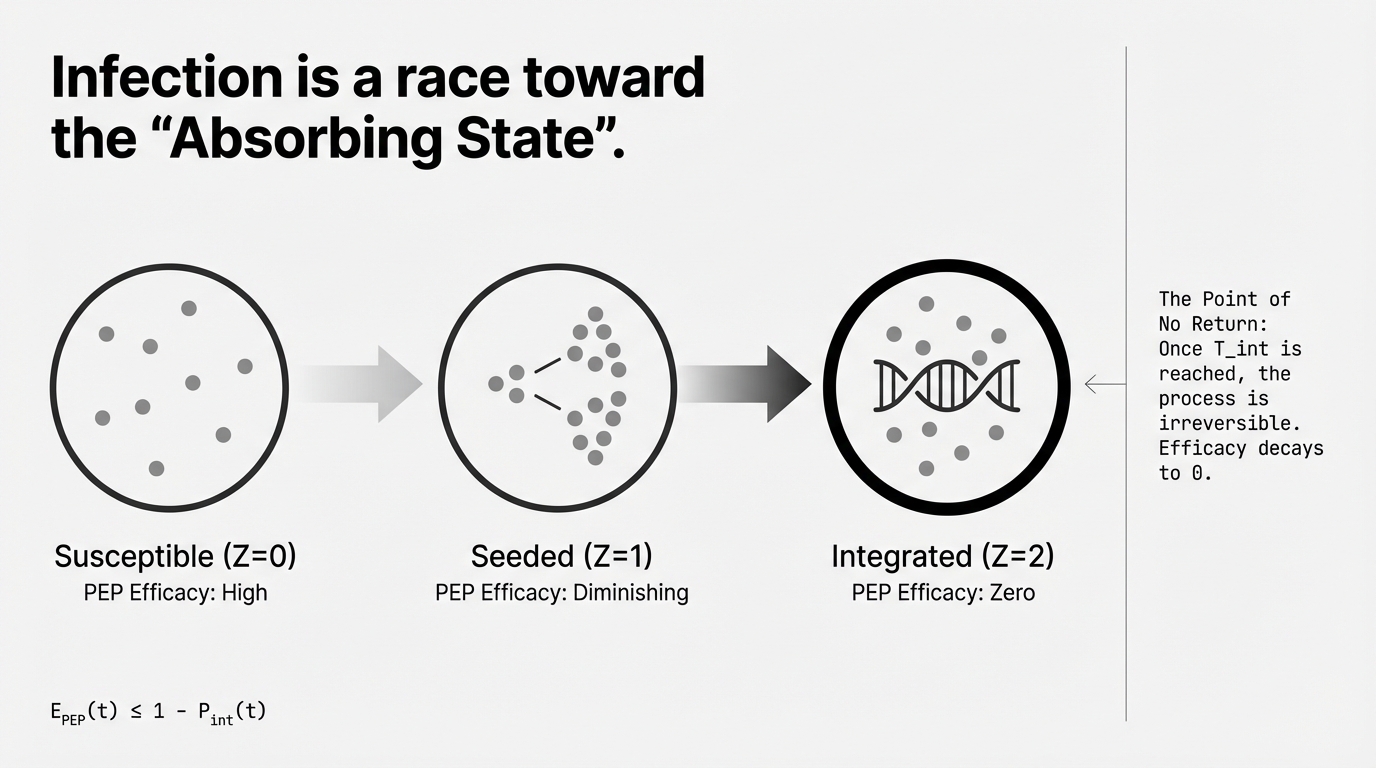
Infection progresses through three states: Susceptible, Seeded, and Integrated. Once proviral integration occurs (Z=2), the process is irreversible. PEP efficacy decays to zero. The critical formula: EPEP(t) ≤ 1 − Pint(t).
Slide 04 — Stochastic Dominance
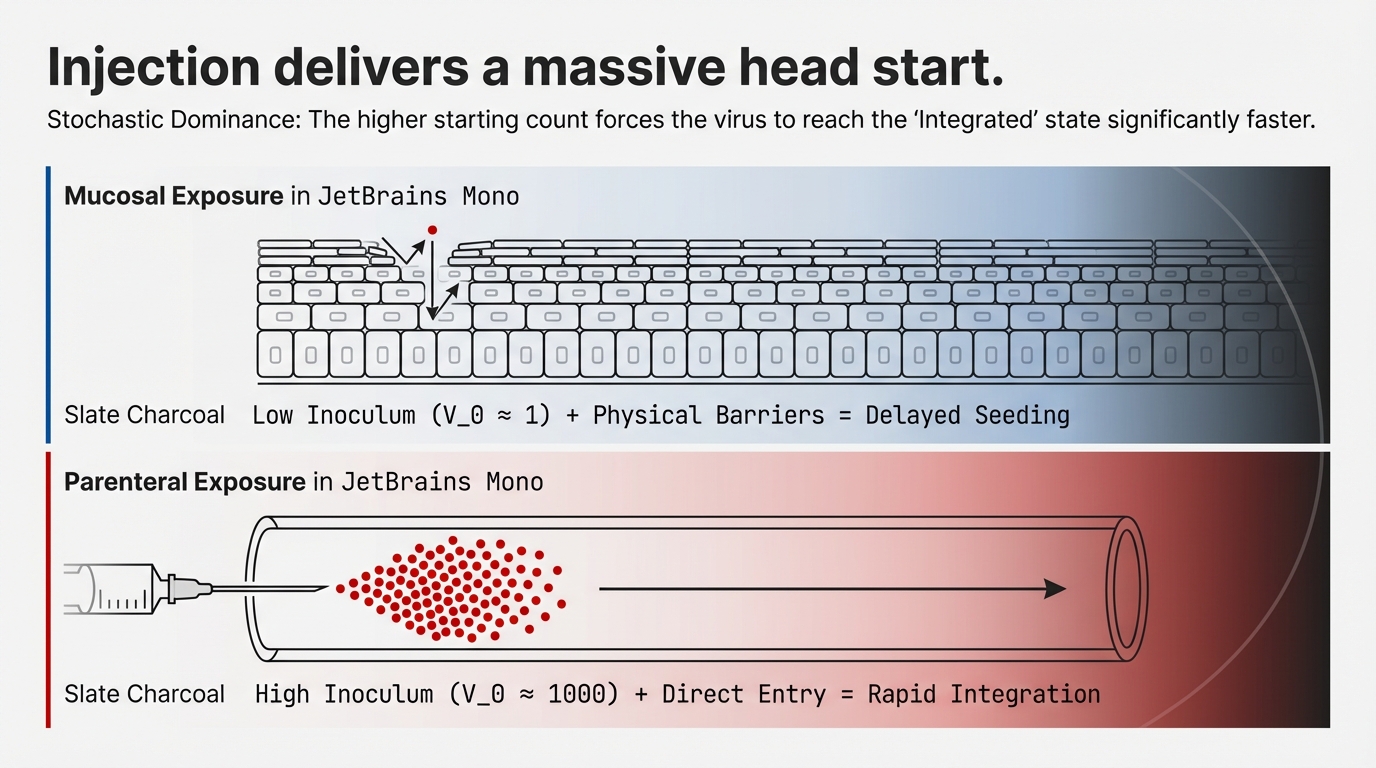
Parenteral exposure bypasses all physical barriers. Mucosal exposure delivers a low inoculum (V0 ≈ 1) that must cross epithelial barriers. Injection delivers a high inoculum (V0 ≈ 1000) directly to the bloodstream, forcing rapid integration.
Slide 05 — The Compression Zone
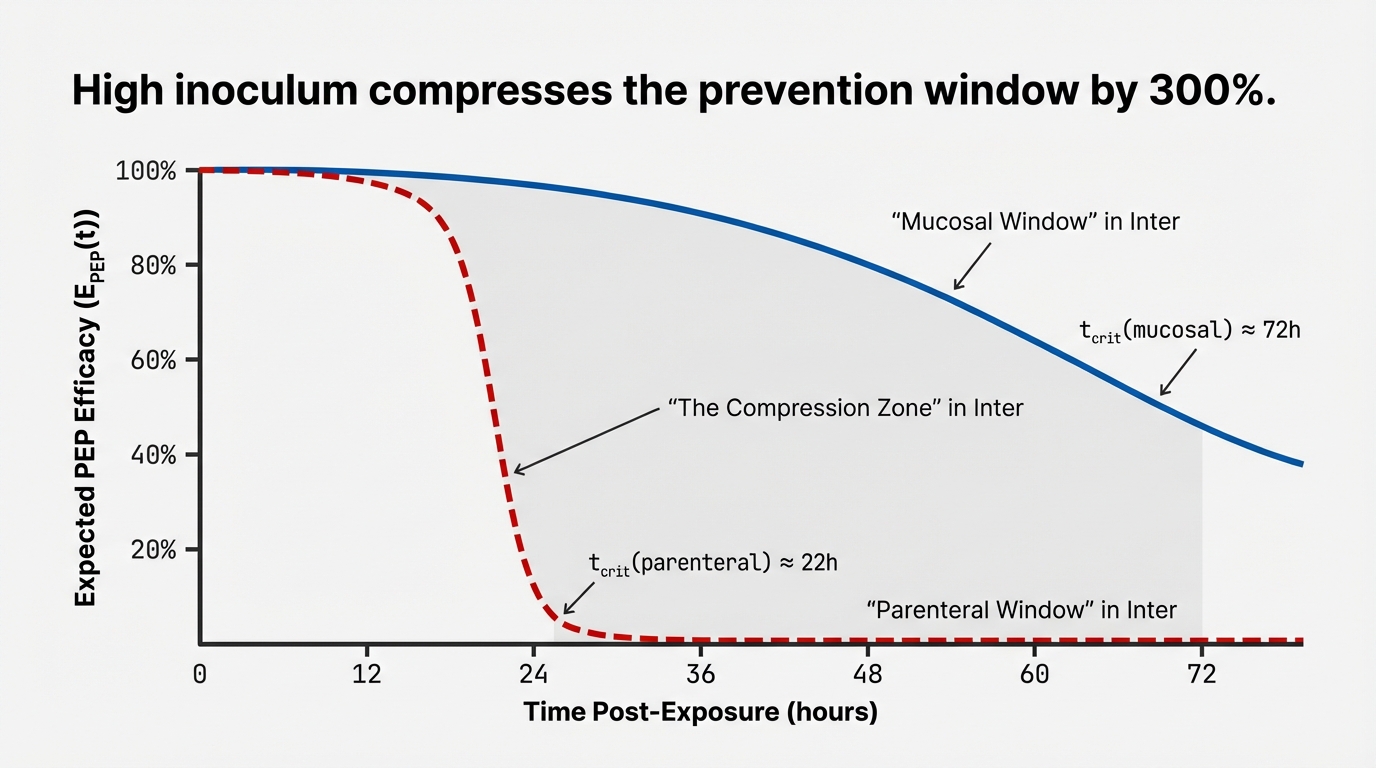
The prevention window compresses by ~3× for injection exposure. The mucosal window (blue, solid) persists to tcrit ≈ 68–76h. The parenteral window (red, dashed) collapses to tcrit ≈ 16–28h. Between ~28 and ~68 hours is the “Compression Zone” — where mucosal PEP still works but parenteral PEP has already failed.
Slide 06 — Experimental Validation
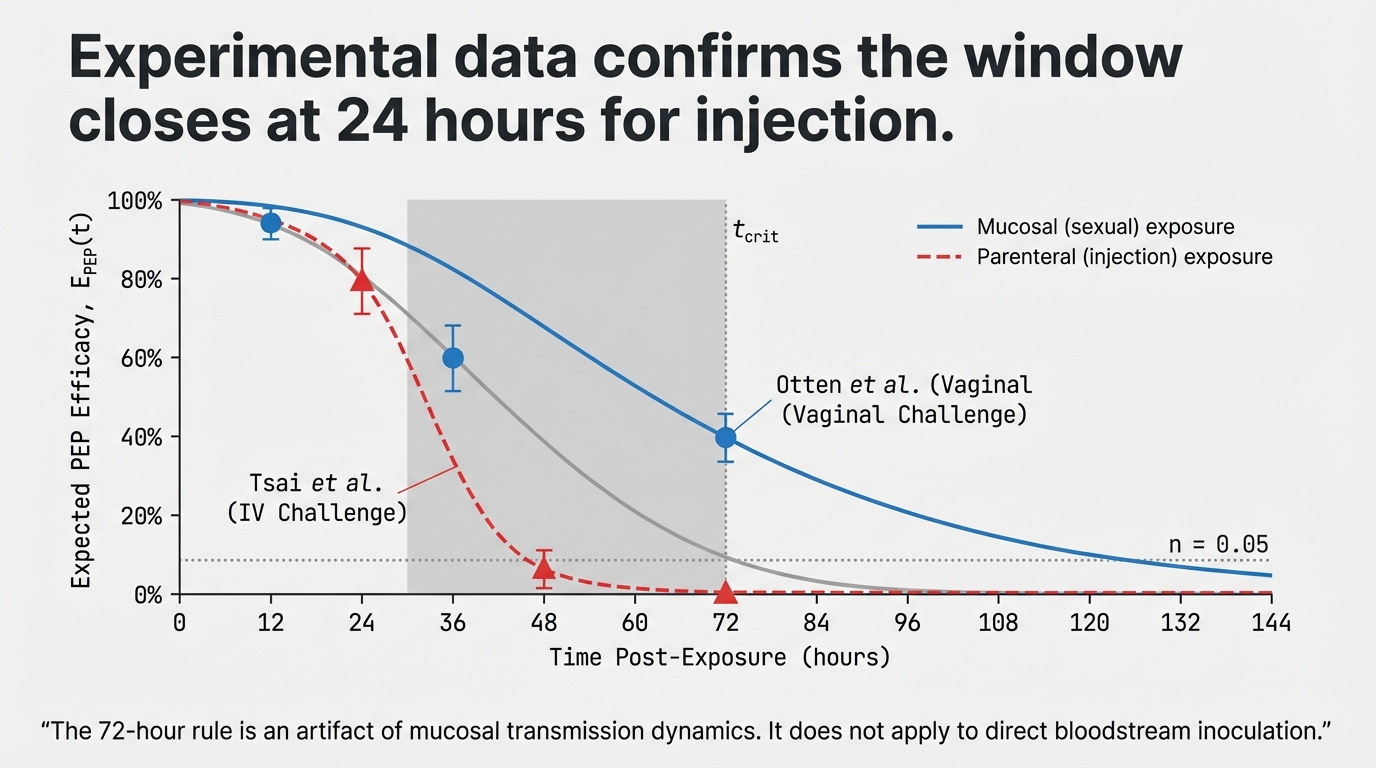
Non-human primate data confirms the model predictions. Tsai et al. (IV challenge) and Otten et al. (vaginal challenge) show the predicted divergence. The 72-hour rule is an artifact of mucosal transmission dynamics — it does not apply to direct bloodstream inoculation.
Slide 07 — The Critical Time
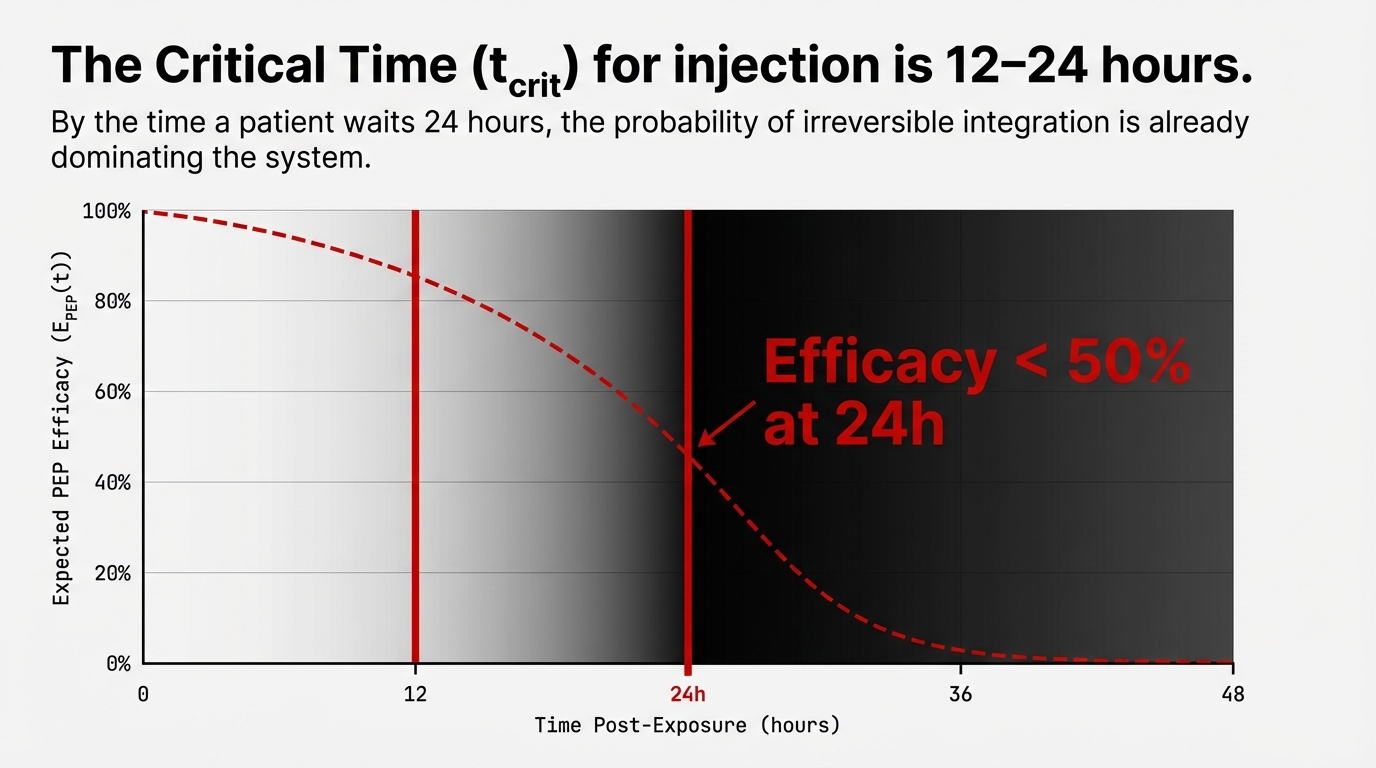
By 48 hours post-injection, PEP efficacy falls below 50% across all source viral loads. The probability of irreversible integration is already dominating the system. The critical intervention window for parenteral exposure is 16–28 hours, not 72.
Slide 08 — Structural Barriers
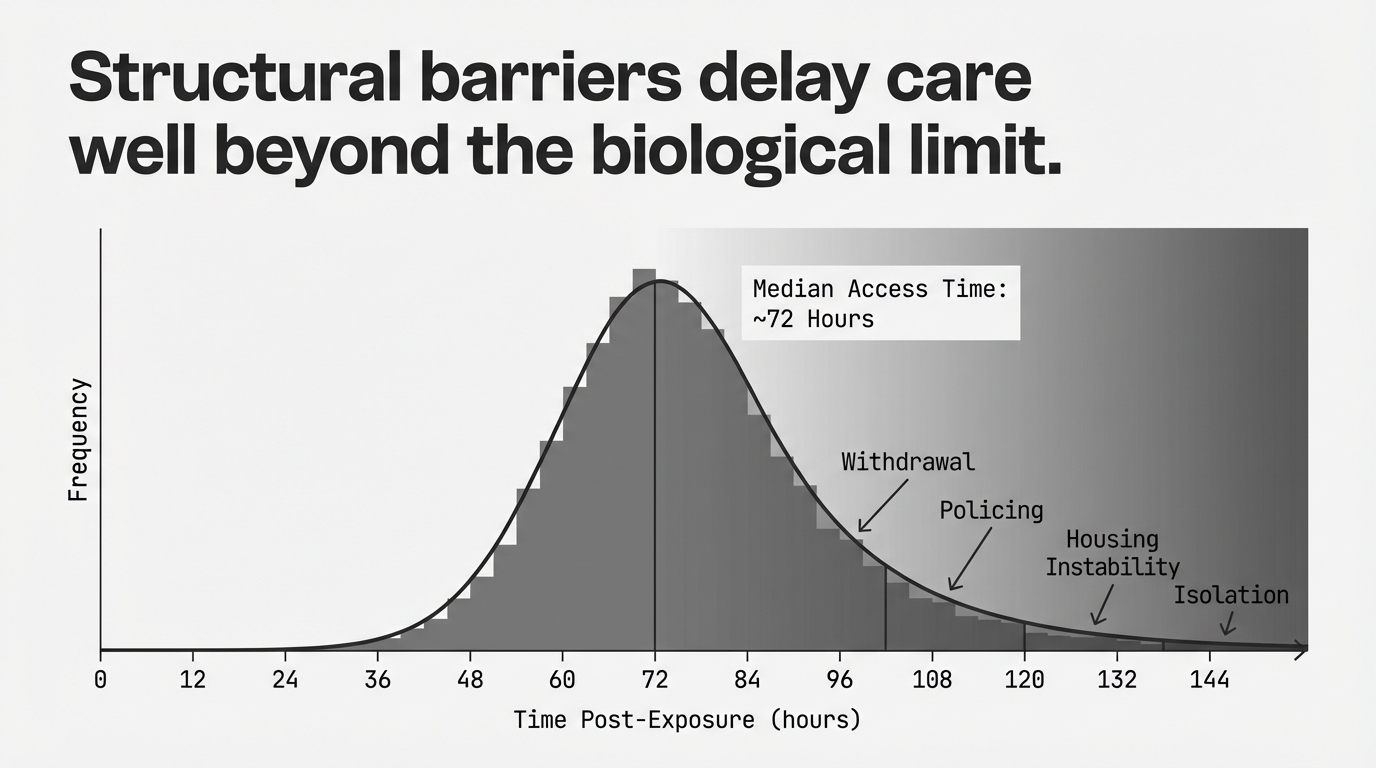
The median PWID access delay is ~72 hours — three times the biological limit. Withdrawal, policing, housing instability, and geographic isolation create structural barriers that push healthcare access well beyond the effective parenteral window.
Slide 09 — The Failure Mode
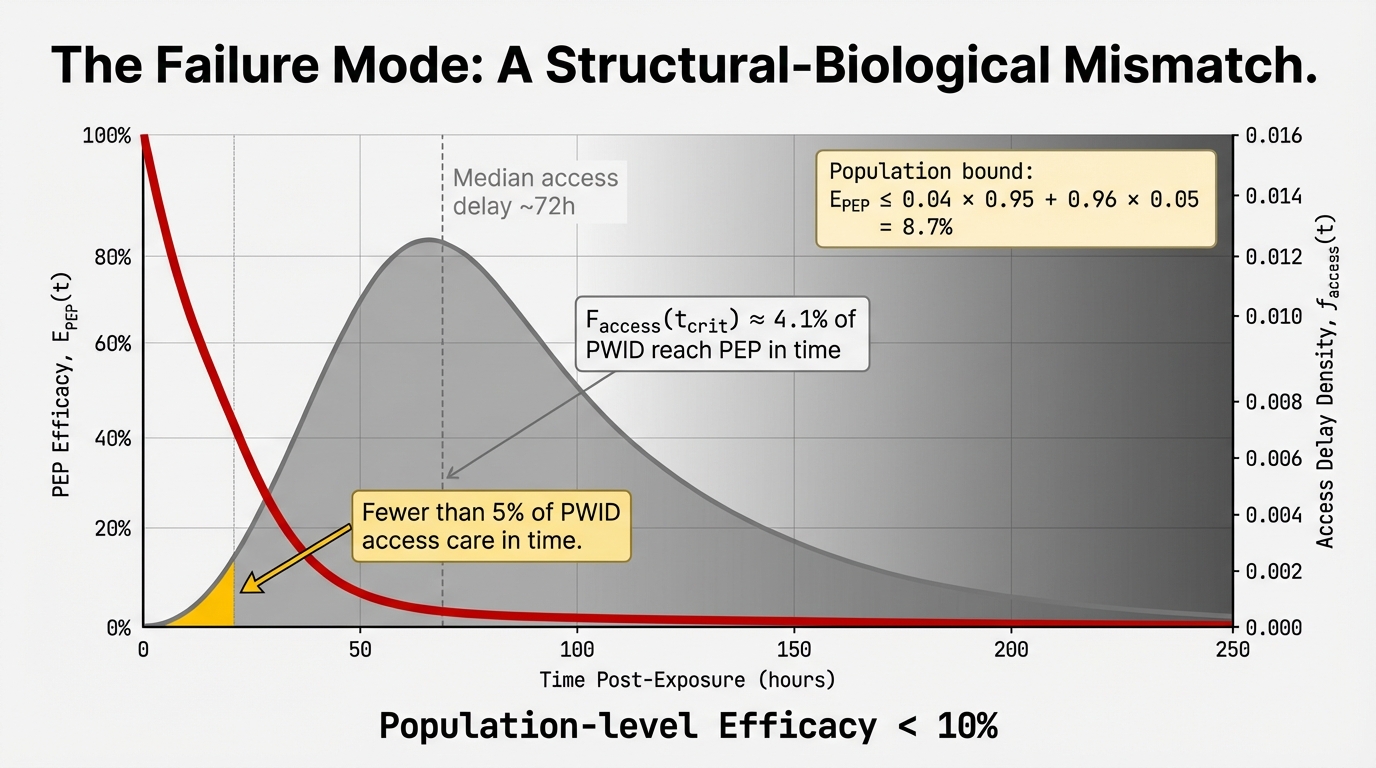
Approximately 2% of PWID access PEP within the effective window. The overlap between the access delay distribution and the efficacy curve yields a population-level bound: E̅PEP ≤ 6.8%. This is a structural-biological mismatch, not a pharmacological failure.
Slide 10 — The Pivot to PrEP
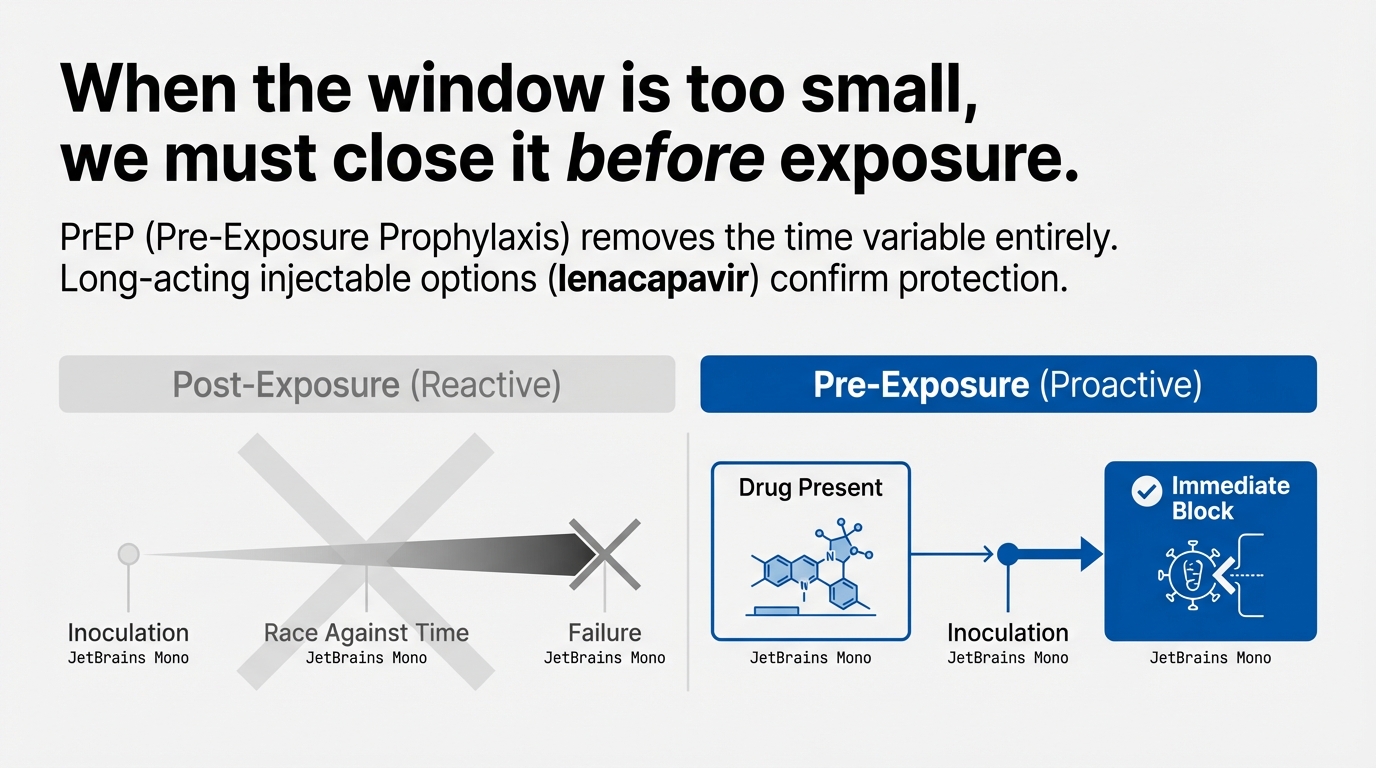
When the window is too small, the only option is to close it before exposure. Pre-exposure prophylaxis (PrEP) removes the time variable entirely. Long-acting injectable options like lenacapavir provide immediate, continuous protection without requiring post-exposure access.
Slide 11 — Summary & Implications
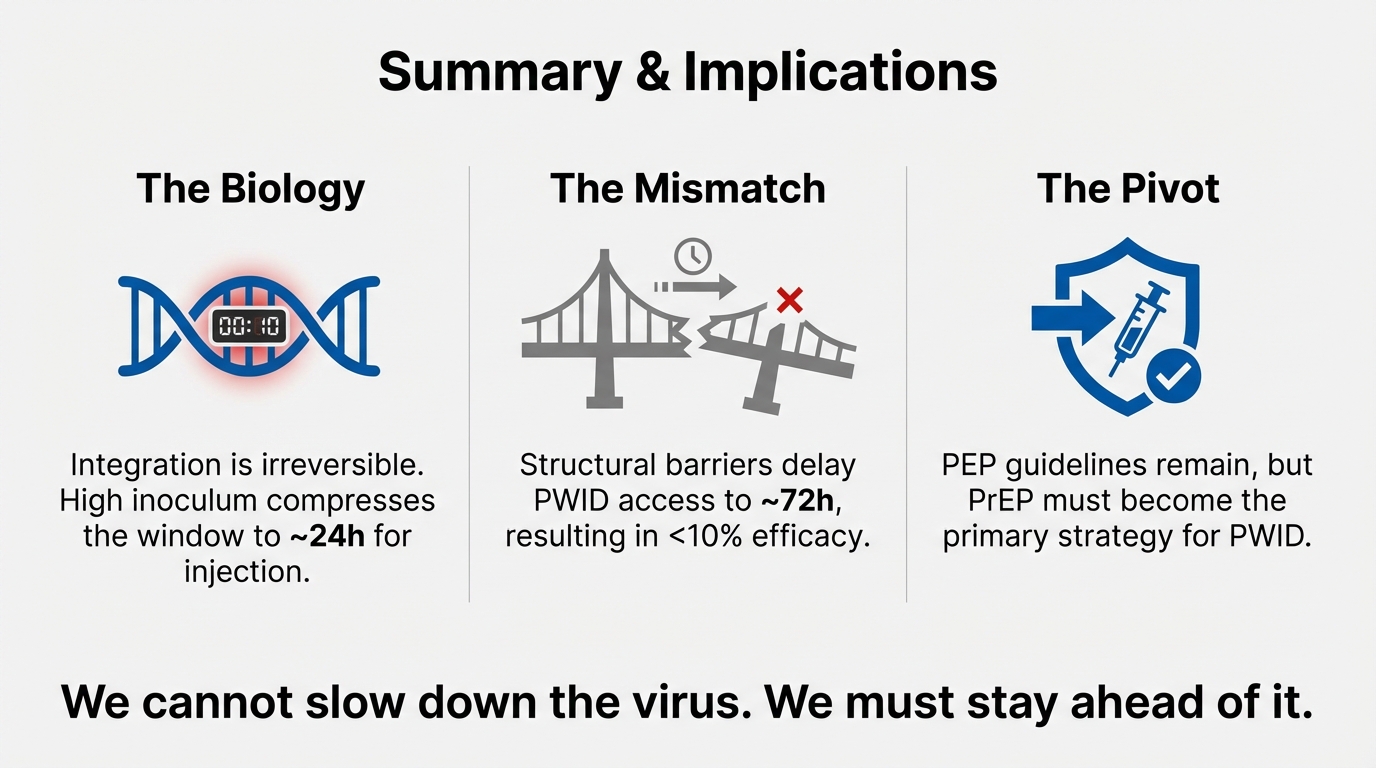
We cannot slow down the virus. We must stay ahead of it. Integration is irreversible and compresses the injection window to ~16–28h. Structural barriers delay PWID access to ~72h, resulting in <10% efficacy. PrEP must become the primary prevention strategy for PWID.

